
By Joe Allbright, Alex Leung, Mitchell Momanyi, Rebecca Owen, and Teresa Winer
Authors’ note: This piece was written before COVID-19 became the public health crisis it is today. The lessons we can draw are still very applicable, however. As the world shifts its focus to combat a pandemic and the consequent economic disruption, we may hear far less about the opioid crisis … but that will not mean it’s gone away. In fact, the current crisis will contribute to some of the factors that worsen substance abuse disorders.
In the thousands of years since poppies were first cultivated, opiates have at times been heralded as medical miracles, condemned as addictive and lethal, and the center of lucrative global trade routes and wars.[IC1] The 21st century’s scientific and pharmacological advances have only made opioids more therapeutic, more addictive, more lethal, and more valuable than ever before.
Because of this complexity, opioids pose a unique challenge to public health. A commitment to further developing opioids as medicines risks the creation of new addicts and allows powerful new forms of the drug to spread. Restricting access will increase the costs, force addicts to other options, and limit the treatment options available to pain sufferers. Striking the right balance is made harder still due to the large financial conflicts of interest in both the licit and illicit opioid markets.
Today’s opioid crisis is a public health emergency of a global scale, but the character of the emergency as well as the nation’s response varies significantly between nations. How a government views opioids—as medicine or vice—will determine whether it responds through social services, law enforcement, or some combination of the two. Depending on the available economic incentives, a government may not respond at all. A lasting solution to the crisis requires a deep understanding of a region’s politics, culture, economics, and health infrastructure.
We assume the reader is likely familiar with the story of opioids in the U.S., so we will focus on how this crisis has affected other nations to identify and share more information that may be helpful to all of us. In Western Europe, we see a focus on harm reduction over deterrence. In Singapore, drug abuse has been well controlled through public education and strong penalties. As Afghanistan’s economy is largely reliant on opium production and trade, its stability may rely on the international demand for opiates. Kenya shows us an example of unintended consequences, where stigmatizing and restricting opioid access apparently prevents pain sufferers from receiving necessary palliative care. Finally, countries in South America today are largely unaffected by opioids but are learning from others should the crisis spread.
Portugal & Switzerland
Western Europe has a history of both medicinal and recreational opiate use stretching back to the Crusades. It has been highlighted by literature and historical archives from the Confessions of an English Opium-Eater, the addiction consequences of the use of morphine for pain relief of wounded soldiers in the wars of the late 19th century, to the depiction of urban drug culture so well portrayed in the novel and subsequent movie adaptation Trainspotting. The governments of Western Europe have adopted a variety of responses to the opioid crisis, which have been met with varying degrees of success and failure. In particular, two countries have implemented policies emphasizing harm reduction rather than harsh deterrence—limiting the prevalence of addiction in the process.
Switzerland in the 1970s had a reputation as a permissive culture, resulting in heavy drug use in public places. The Zurich parks became a nightmarish scene the New York Times dubbed a “bazaar of the bizarre.”[PS1] The initial reaction was to increase enforcement and adopt stiff sanctions for possession, consumption, and sale of illicit narcotics. At the same time, Switzerland adopted a tolerant stance on consumption within controlled areas. By the end of the 1980s, despite these measures, Switzerland still had an enormous, widespread drug problem. The public health consequences were becoming even more severe due to the spread of HIV among intravenous drug users. The prevalence of HIV was estimated to be the highest in Western Europe.
The ever-pragmatic Swiss decided to rethink their position, starting with support and coordination of direct service organizations that were running needle exchange programs and safe injection sites. The success of these initial efforts spurred the formation of a series of heroin-assisted treatment trials in the 1990s, which included the prescription of heroin for controlled consumption for addicts.[PS2]
The evidence collected from these trials helped to direct the next development in the drug treatment in Switzerland, known as the four-pillar model (policing, prevention, treatment, harm reduction). By keeping these core principles together as a cohesive vision, this program was able to gather support from a larger group of stakeholders.[PS3] In 2008 a public referendum adopted the four pillars in all cantons, a remarkable unity of support for a program that included the sometimes-controversial “harm reduction” as a part of the program. Between 1991 and 2010, overdose rates halved, HIV infections decreased by 65 percent, and new heroin users decreased by 80 percent[PS4] The four pillars formed a consistent organizing principle, and local governments were given the responsibility to develop specific programs. As social solutions need to evolve and adapt with circumstances, local control allowed these programs to respond quickly.
In the 1990s, Portugal had an opioid problem so severe that it was called the heroin capital of Europe.[PS5] Nearly 10 percent of the population used heroin, and in 1999 approximately 1 percent of the population reported an addiction to hard drugs.[PS6] The country had the highest rates of drug-attributed AIDS deaths during this period. Prisons were crowded, violent crime was rampant, and social issues were severe.
To combat this, Portugal passed a series of laws that went into effect in 2001. Possession of small amounts of narcotics for personal use was decriminalized, though dealers were still charged and jailed. Instead of prison, drug users went before a three-person commission for assessment. This “dissuasion” commission, still in effect today, typically consists of a lawyer plus two health care professionals and determines what next steps are best for the person.[PS7] If a person is determined to be an addict and agrees to seek help, penalties are suspended for six months. Portugal also added 40 rehabilitation clinics with a focus on returning people to good health through activities and engagement.[PS8] For those not ready for rehab, a coordinated network of outreach groups was established to visit drug users in the community, keep communication lines open, and to offer a path out of addiction. In Lisbon, mobile methadone units bring care to users where they live and work.
Though economic challenges have tempered the funding for this work, the results have been so marked that the program has become a case study for other governments as they combat the opioid crisis. Overdose deaths decreased by over 80 percent between 1999 and 2015.[PS9] The contribution of drug-related causes in new AIDS cases fell from 52 percent to 6 percent and drug-related incarceration fell by 43 percent.[PS9]
Singapore
Singapore, like most developed economies, is rapidly becoming an aging society. In particular, the proportion of residents aged 65 years and older has increased from 8.7 percent in 2008 to 13.7 percent in 2018,[S1] with about one in 10 people suffering from chronic pain.[S2] The number of people with chronic pain conditions is expected to increase, resulting in greater demand for opioid analgesics.
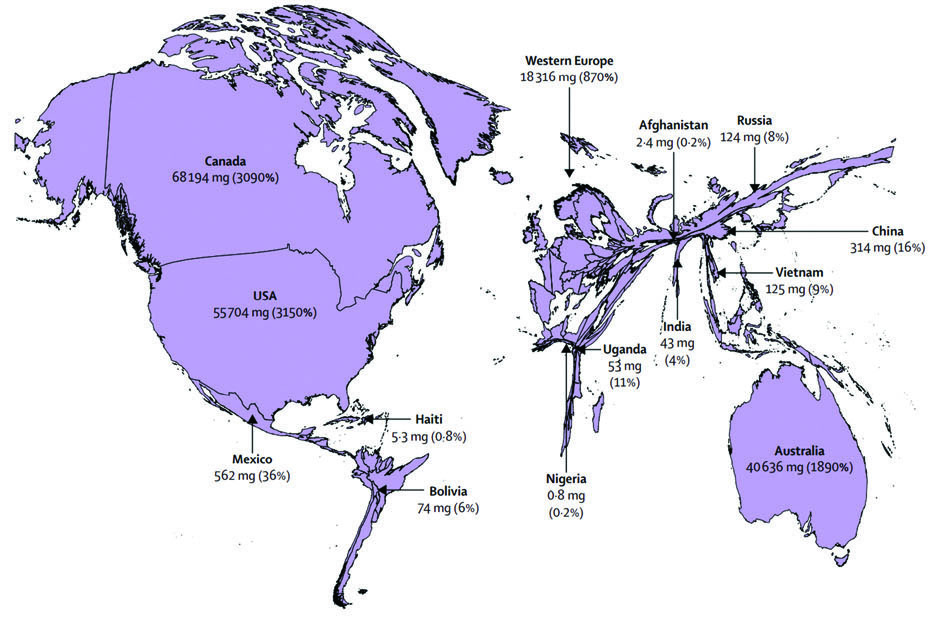
According to statistics from the University of Wisconsin Pain & Policy Studies Group, the per capita consumption of opioids in Singapore doubled between 2005 and 2010.[S3] Although the consumption has grown, there is a relatively low opioid use in Singapore. Specifically, its consumption of opioids in 2009 was only 4.5 mg morphine equivalent per person; this is 13 times lower than the global average, and 160 times lower than the United States’ consumption at the time.[S4]
Singapore is one of the few countries to have kept opioid abuse and addiction under control. Singaporean law allows doctors the discretion to prescribe controlled drugs with no restrictions on amount or length of prescription. Government and community groups have worked closely with related parties on raising general public awareness of safe opioid use and the harm and consequences of opioid abuse.
The Pain Association of Singapore has developed guidelines on how to prescribe opioids and monitor patients,[S5] which have been widely adopted by the medical community. These guidelines advise doctors to set an agreement with their patients regarding the terms of opioid administration; in general, patients will be put on a trial for one or two months under close monitoring prior to any dosage or medication changes. Doctors are advised to be on alert for patients who may show signs of addiction such as asking for increased dosages or “doctor-shopping.” The Singapore Ministry of Health has recently released and sought feedback on its Draft National Guidelines for the Safe Prescribing of Opioids[S6] that contains sections including: “Acute Pain,” “Chronic Non-Cancer Pain,” “Cancer Pain and Pain in Life-Limiting Non-Cancer Diseases,” “Non-Pain Indications,” and “Opioid Addiction.”
Moreover, Singapore’s tough laws and enforcement that involve potential capital punishment have served as strong deterrents against illicit drug sales and consumption. This stringent oversight reduces or eliminates access to opioids through prohibited channels and thereby lowers the potential of opioid abuse and addiction.
Afghanistan
Ninety percent of the world’s heroin supply originates in the poppy farms of rural Afghanistan.[A1] While the region, now known as the golden crescent, has a history of opium production dating back to the East India Company, it was only during the 1950s, after production was made illegal in Iran, that Afghanistan became the center of Middle Eastern opium production. In the decades since, the opium economy has grown into a multi-billion-dollar industry. In 2017, the footprint of opium production in Afghanistan could cover the state of Rhode Island. Farming alone provides the equivalent of 590,000 full-time jobs.[A2] Depending on growing conditions, the production and trafficking of opium is responsible for 10 percent to 30 percent of Afghanistan’s GDP.
Rural Afghanistan—destabilized by war; lacking effective governance, security, and infrastructure; and without similarly profitable licit industries—presents the perfect conditions for an opium economy to take hold. International pressure, Taliban restrictions, and drought have been able to suppress production for a year or two, but without enforcement or viable alternatives the industry tends to re-emerge stronger than ever. Besides the farmers themselves, there are many entrenched interests looking to support the opium economy. Taxes are paid to the Taliban, insurgent, and antigovernment groups. Ushr, a traditional tithe on agricultural production, is directed toward charitable and religious groups.[A3] Efforts to eradicate opium production in areas only deepens the poverty, drives people into insurgent groups, and increases production elsewhere.[A4] A piece by the Brookings Institution says it best: “There is simply nothing in Afghanistan that produces more jobs than the opium poppy economy, or could do so in the foreseeable future.”[A5]
While opium is an economic boon to many Afghan groups, a combination of ready access and desperation has driven millions into addiction. A 2015 survey estimates there are 3 million drug users in Afghanistan, with opium and heroin by far the most common. Over 30 percent of households were directly affected by drug use—16.1 percent of men, 9.5 percent of women, and 9.2 percent of children 14 and under.[A7] Afghan and international groups have established drug treatment centers, but the capacity would only cover about 10 percent of opium users. Furthermore, the majority of these centers are exclusively for men.[A7] Some Taliban groups have been setting up makeshift rehabilitation centers in mountain caves. The treatment consists of months of long walks and cold showers, and many of those treated are later recruited as fighters.[A8]
There is no clear solution to this problem. World demand for opiates is higher than ever; neither Afghan nor United Nations resources have been able to curb supply or keep up with the rate of addiction. Poverty facilitates the creation of addicts, addiction increases poverty, and the best way to escape this cycle is through producing or trafficking opium. Unlike other nations, Afghanistan does not have the ability to combat opioids as if they were some external threat to be eliminated; the opium economy is so deeply integrated into the fabric of their society it will require years of carefully coordinated effort before the country can begin to break free.
Kenya
In Kenya, there are two contrasting stories related to the distribution and use of opioids. The first relates to a history of constrained access to palliative care drugs such as morphine, despite the increased need for narcotic drugs as rates of non-communicable diseases rise. On the other hand, Kenya continues to grapple with the problem of heroin smuggling, especially via its sea ports in the coastal region.
Much has been written about the widespread prevalence and abuse of opioids in the past two decades in high-income countries—particularly in the United States, Canada, and Australia. The picture is far different in developing nations, where the supply of opiate analgesics is far below the medical need for pain relief.[K1]
In Kenya, there are several factors that prevent patients in need of palliative care from accessing the treatment they need. Because morphine is designated as a controlled substance, there is fear by medical practitioners to prescribe it. Dr. Zipporah Ali, a leading pain specialist in Nairobi, Kenya, states that “this fear—along with punitive laws, poverty, stigma, cost and health care providers’ lack of knowledge and skills—continues to be a barrier to access to pain relief.”[K2]
International treaties aimed at reducing the spread of illicit drugs[K3] have limited access to those who have legitimate need. The cost of drugs such as morphine is significantly higher in Kenya than in international markets;[K4,K5] and a survey of Kenyans on drug access for non-communicable diseases highlighted that drugs at private pharmacies were significantly more expensive than those provided at government facilities.[K6] Kenya’s health system requires patients to pay for a significant portion of these high drug costs—particularly those with chronic conditions that require regular medication. Furthermore, patients may face indirect costs due to transportation and forgone wages in order to search for the best prices.
Social stigma is a key cultural aspect that can constrain access to opioid analgesics. According to research on how drug regulations affect access to controlled medicines, “use of morphine and other opioids for pain relief, for example, is heavily stigmatized in Armenia, Kenya, and many other low- and middle-income countries.”[K7] Underlying this stigma is the stereotyping of drug abusers as criminals and societal failures. In Kenya, drug abuse is rarely viewed as being primarily a medical disorder. As a result, there is a tendency among providers to overcorrect for the potential of drug dependency when prescribing narcotics. Patients in need of these drugs are often prescribed less than optimal amounts and may also incur long wait times to receive the drugs that they need.
While Kenya still has very few pain specialists—a recent government study on the health care profession lists only one palliative care doctor out of 2,089 specialists[K8]—there have been some positive developments. Palliative care has been integrated into the curricula of all medical and nursing schools in the country, ensuring that medical practitioners across a broad spectrum of specialties are familiar with the basics of pain management. The country’s leading palliative care association, Kenya Hospices and Palliative Care Association (KEHPCA), plays a key role in advocating on behalf of chronically ill patients in need of quality pain treatment. KEHPCA is working with the government to integrate palliative care into most public hospitals and clinics. The association has also recently partnered with Kenya’s largest referral hospital, Kenyatta National Hospital, to boost supplies of oral morphine by having some of the supply produced locally.
Aside from the limited access to opioid analgesics, Kenya is also dealing with abuse spurred by its centrality as an international trade hub for heroin. For the past several years, Eastern Africa has been an important hub for heroin smuggled from parts of Asia and destined for North America and Western Europe.[K9] In August 2014, the Kenyan government seized and destroyed a 374-kilogram shipment of heroin valued at about USD 12.5 million.[K10] Although such seizures get the most media attention, a significant amount of the drug is smuggled through other mechanisms such as small boats and roads. In an analysis of the policing of heroin trade routes in Eastern Africa, political scientist Margarita Dimova states that “dirt roads, as well as major international arteries, are increasingly used to avoid maritime interception and make use of the many porous land borders in the region.”[K11]
Of the smuggled heroin that remains in the region, its social and health impacts include:
- A higher risk of contracting infectious diseases such as HIV/AIDS through the sharing of needles used to inject the drug;
- Increased pressure on the country’s public health system that was designed to fight the spread of infectious diseases and is struggling to address substance abuse;
- Reduced productivity among the working-age population; and
- Increased crime such as petty theft carried out in order to sustain addiction.
These impacts can reinforce each other, resulting in a vicious cycle for the individual and society. For instance, a young individual of working age may resort to heroin abuse to deal with depression brought about by unemployment. They may resort to stealing from their family in order to sustain the habit, thus landing them in prison. The resulting prison time may make it even more difficult for the individual to attain gainful employment.
While the use and abuse of opioids is well documented and detailed data exists for many countries in Europe and North America, there is still much data missing for countries such as Kenya. Good-quality data is needed to help policymakers better understand the issue and devise helpful responses to both current and emerging social and health issues.
Brazil
As previously indicated, the United States is currently the center of the global opioid crisis. Canada, Mexico (primarily along the U.S. border), and some Caribbean nations have seen a sharp increase in opioid use.[B1] As we move farther south, away from the U.S.-bound trade routes and culture of over-prescription, both licit and illicit opiate use drops off significantly. In most of South America, heroin use is hardly measurable and prescription opioid abuse is estimated to be only 0.2 percent among adults aged 15-64.[B2]
The region is no stranger to the economics of drug addiction. Brazil is often the gateway between South America’s cocaine production and European and West African markets. It’s surprising that opioid abuse has not taken root in Brazil given that it has the world’s highest rates of violent crime, deep wealth inequality, organized trafficking networks, and the world’s fourth-highest incarcerated population.[B3] Paradoxically, it may be the relative abundance and low cost of cocaine, crack, and marijuana that prevent opioids from gaining a foothold.
Though rates of opioid addiction are low today, the global crisis presents a clear threat to the region. The stable system in place now—low demand deters traffickers, lack of access lessens addiction—may be upended by powerful and easily transported synthetic opioids like fentanyl. Brazil is carefully watching its neighbors. To the north, U.S.-bound heroin production in Colombia is increasing. To the west, Chile’s rate of opioid use increased from 0.3 percent to 1.2 percent within only four years. To the south, Uruguay’s policy of drug decriminalization and legalization may undermine efforts to keep opioids out.[B4]

While the rest of the world is directing their efforts toward policing, harm reduction, and recovery, Brazil’s focus today is on prevention. In general, it’s harder to find funding for prevention efforts before the need is obvious—at which point it is often too late.[B4] As with Kenya, though, such efforts to monitor and stigmatize opioids may end up creating barriers for pain sufferers. “Opiophobia” may be creating a crisis of opioid under-prescription in Latin America.
Brazil must walk a narrow path, cautioning physicians to prescribe opiates responsibly while avoiding the spiral into addiction that so many other nations have succumbed to. To accomplish this, it will need to collect reliable and timely data, develop coordination between medical and drug policy, and learn from the experiences of other health systems struggling with the same challenges.
Conclusion
The opioid crisis is a fire that has spread across the globe. Some areas are battling the heat, some the smoke; one unaffected region may be trying to combat the spread while another is just trying to stay warm. Within each of our neighborhoods there are similar pockets of affected and unaffected groups. A multifaceted problem such as this one is likely to require a multifaceted response, and we only need to look to our global neighbors to see how other approaches have (or have not) succeeded across varying cultural and political settings.
The total cost of this crisis has been astonishing. Tens of millions of lives have been affected,[IC2] record profits have been made and lost, health systems and social safety nets have been stressed to the point of breaking.
Actuaries are trained to evaluate risk—both the risk of action and the risk of inaction. The opioid crisis is a perfect example of a situation that could benefit from our unique insight, and a potential model for how other public health crises might emerge. Actuaries can spot trends in the data while the cost of intervention might still be low; to predict the first-, second-, and third-order effects of a response; and to ensure that our current systems are built to resist this sort of a disaster in the first place.
JOE ALLBRIGHT, ALEX LEUNG, MITCHELL MOMANYI, REBECCA OWEN, and TERESA WINER are members of the Academy’s Health Practice International Committee.
References
Intro/Conclusion References
[IC1] “Opium—A History”; The New York Times; 1996. [IC2] “Information sheet on opioid overdose”; World Health Organization; August 2018.Switzerland References
[PS1] “Zurich Journal; A Marketplace for Drugs, a Bazaar of the Bizarre”; The New York Times; September 27, 1990. [PS2] “Switzerland couldn’t stop drug users. So it started supporting them.”; North Carolina Health News; January 21, 2019. [PS3] “The Swiss Four Pillars Policy: An Evolution From Local Experimentation to Federal Law”; The Beckley Foundation Drug Policy Programme; May 2009. [PS4] “Inside Switzerland’s Radical Drug Policy Innovation”; Stanford Social Innovation Review; July 22, 2019Portugal References
[PS5] “How Portugal is solving its opioid problem”; American Psychological Association. [PS6] “Lessons from Portugal: The Case for Drug Policy Reform”; Beckley Foundation; April 2018. [PS7] “Portugal: Country Drug Report 2019–Drug laws and drug law offences”; European Monitoring Centre for Drugs and Drug Addiction; 2019. [PS8] “How Europe’s heroin capital solved its overdose crisis”; CBC. [PS9] “Drug Decriminalization in Portugal: Learning from a Health and Human-Centered Approach”; Drug Policy Alliance.Singapore References
[S1] “Population Trends”; Singapore Department of Statistics. [S2] “Draft National Guidelines for the Safe Prescribing of Opioids”; Singapore Ministry of Health. [S3] “New guidelines on prescribing strong painkillers”; The Straits Times. [S4] “Life Before Death Press Release Annex B”; Lien Foundation. [S5] “New guidelines on prescribing strong painkillers”; The Straits Times. [S6] “Online Consultation on Draft National Guidelines for the Safe Prescribing of Opioids”; Singapore Ministry of Health.Afghanistan References
[A1] “How the US military’s opium war in Afghanistan was lost”; BBC News; April 25, 2019. [A2] “Afghanistan opium survey 2018: Challenges to sustainable development, peace and security”; United Nations Office on Drugs and Crime; July 2019. [A3] “Afghanistan opium survey 2017: Challenges to sustainable development, peace and security”; United Nations Office on Drugs and Crime; May 2018. [A4] “Afghanistan’s Opium Poppy Economy”; Middle East Institute; April 20, 2012. [A5] “Afghanistan’s opium production is through the roof—why Washington shouldn’t overreact”; Brookings Institution; November 21, 2017. [A6] “Opium use booms in Afghanistan, creating a ‘silent tsunami’ of addicted women”; Washington Post; June 19, 2017. [A7] “2015 Afghanistan Drug Report”; United Nations Office on Drugs and Crime; December 9, 2015. [A8] “Afghanistan drug addiction on the rise as conflict continues”; Al Jazeera; February 7, 2020.Kenya References
[K1] “Alleviating the access abyss in palliative care and pain relief—an imperative of universal health coverage: the Lancet Commission report”; The Lancet; October 12, 2017. [K2] “In Kenya, Overcoming Drug Fears to Expand Access to Palliative Care”; Open Society Foundations; April 20, 2016. [K3] “The International Drug Control Conventions”; United Nations Office on Drugs and Crime; 2013. [K4] “The Market Price Index Survey Results”; Public Procurement Regulatory Authority; 2018. [K5] “International Medical Products Price Guide”; Management Sciences for Health; 2015. [K6] “Perceptions of Kenyan adults on access to medicines for non-communicable diseases: A qualitative study”; PLOS ONE; August 24, 2018. [K7] “How Drug Control Policy and Practice Undermine Access to Controlled Medicines”; Health and Human Rights Journal; June 2017. [K8] “The Status of Healthcare Professionals in Kenya, 2015”; Kenya Ministry of Health; 2015. [K9] “Drug Trafficking Patterns to and from Eastern Africa”; United Nations Office on Drugs and Crime. [K10] “Sh1.3bn drugs ship blown up at sea”; Daily Nation; 2014. [K11] “A New Agenda for Policing: Understanding the Heroin Trade in Eastern Africa”; European Consortium for Political Research; 2014.South America References
[B1] “World Opioid and Substance Use Epidemic: A Latin American Perspective”; Psychiatric Research & Clinical Practice; January 24, 2019. [B2] “World Drug Report 2019”; United Nations; June 2019. [B3] “Drugs and Drug Trafficking in Brazil: Trends and Policies”; Brookings Institution; 2016. [B4] “Crano talks drug prevention strategies in a country ravaged by opioids”; Claremont Graduate University; October 29, 2018. [B5] “Latin American Pain Federation position paper on appropriate opioid use in pain management”; Pain Reports; May 21, 2019.

